Pain Management Functional Goal Calculator
Your Current Status & Goals
Your Results
Complete the form and click calculate to see your personalized assessment and recommendations.
For decades, the medical world operated under a single, dangerous assumption: if you want to stop pain, you must eliminate it completely. The goal was zero. If a patient rated their pain as a 2 out of 10, they were still considered a failure of treatment. This approach led to skyrocketing opioid prescriptions, severe side effects, and patients who were physically numb but functionally disabled. They couldn't walk, work, or enjoy life because they were too sedated to move.
That era is over. The modern golden rule of pain management is not about chasing a magic number on a pain scale. It is about improving function and quality of life, even if some pain remains. In clinical terms, this shift is known as moving from a biomedical model to a biopsychosocial model of care. It acknowledges that pain is not just a signal from damaged tissue; it is a complex experience shaped by your biology, your psychology, and your social environment.
The Shift from Cure to Function
To understand why this rule matters, you have to look at what "pain" actually is. For years, we treated pain like a volume knob. Turn it down, and the problem is solved. But chronic pain is more like an alarm system that has gotten stuck. The fire might be out (the initial injury has healed), but the siren keeps blaring because the brain’s threat detection center is hypersensitive.
If you try to silence the siren with heavy medication, you might get quiet, but you also lose the ability to hear other important sounds-like fatigue, nausea, or cognitive fog. The new golden rule prioritizes what you can do over how much it hurts. Can you play with your kids? Can you return to work? Can you sleep through the night? These are the metrics that matter now.
This approach relies heavily on multimodal analgesia, which means using a combination of treatments rather than relying on one drug class. Instead of loading up on opioids, a doctor might combine physical therapy, nerve blocks, antidepressants for nerve pain, and cognitive behavioral techniques. Each tool targets a different part of the pain pathway, allowing for lower doses of each and fewer side effects.
Why "Zero Pain" Is a Dangerous Goal
Chasing zero pain often leads to the "opioid trap." Opioids are powerful tools for acute pain-like after surgery or a broken bone-but they are poor long-term solutions for chronic conditions like arthritis or fibromyalgia. When used chronically, they can cause hyperalgesia, a condition where the nervous system becomes *more* sensitive to pain, requiring higher doses to achieve the same effect. This creates a vicious cycle.
Furthermore, the fear of pain itself becomes a source of suffering. This is called kinesiophobia-the fear of movement. Patients who believe that any pain means further damage will avoid activity. This avoidance leads to muscle weakness, joint stiffness, and deconditioning, which actually causes more pain when they do move. The golden rule breaks this cycle by encouraging gradual exposure to movement, teaching the brain that motion is safe.
- Avoid all-or-nothing thinking: Accept that some days will be harder than others.
- Pace your activities: Do not "push through" pain to make up for bad days, nor do you need to rest entirely on good days.
- Focus on output, not input: Measure success by steps taken or tasks completed, not by pain levels.
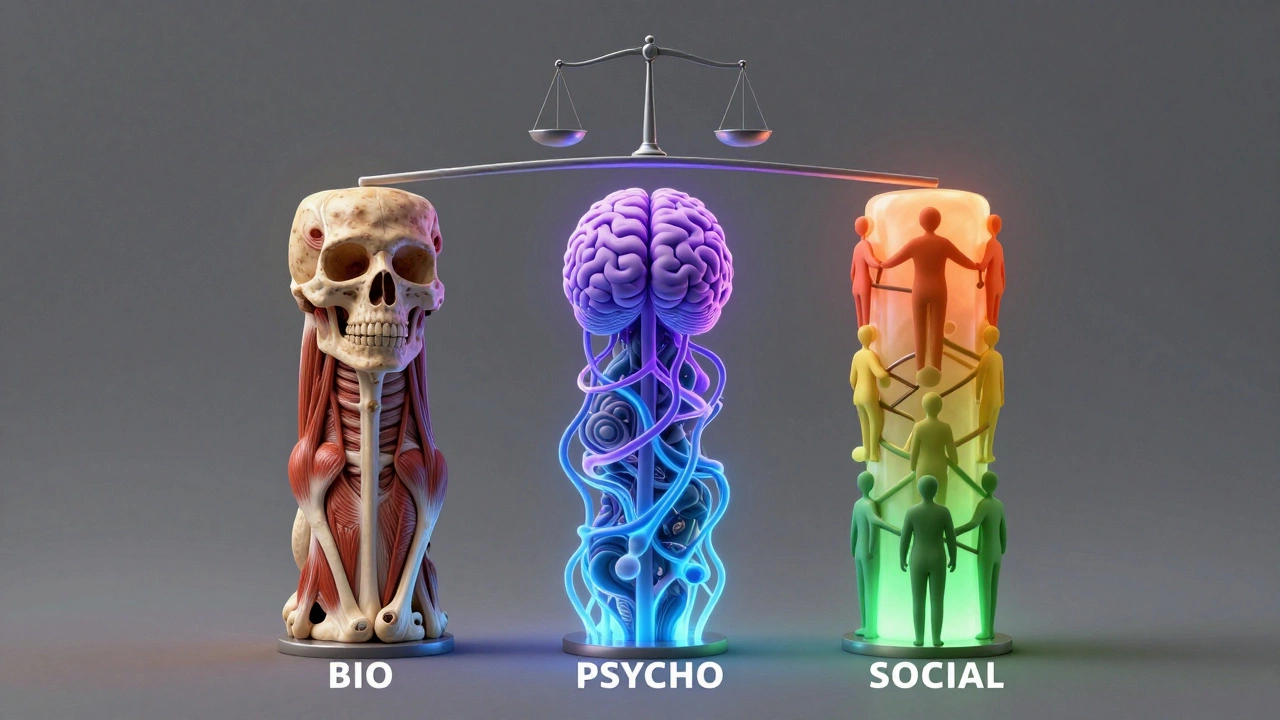
The Biopsychosocial Model in Practice
The biopsychosocial model is the framework that supports the golden rule. It suggests that three pillars influence your pain experience:
- Bio: The physical injury, inflammation, or nerve damage.
- Psycho: Your thoughts, emotions, stress levels, and coping mechanisms.
- Social: Your support network, work environment, financial stress, and cultural beliefs about pain.
Imagine two people with identical knee replacements. Person A lives alone, has high job stress, and believes pain is a sign of weakness. Person B has strong family support, practices mindfulness, and views pain as an annoyance rather than a disaster. Studies consistently show that Person B will likely have better functional outcomes and report less disability, despite having the same biological hardware. This isn't to say the pain is "in your head." It is to say that your brain's interpretation of the pain signal determines its impact on your life.
Treating only the "Bio" pillar is like trying to fix a leaking roof by mopping the floor. You need to address the psychological and social factors too. This might involve seeing a therapist trained in pain management, joining a support group, or making ergonomic changes at work.
Multimodal Analgesia: Building Your Toolkit
Since no single treatment works for everyone, the golden rule encourages building a diverse toolkit. This is often referred to as a stepped-care approach. Here is how different interventions fit into the puzzle:
| Strategy Type | Examples | Primary Benefit |
|---|---|---|
| Physical | Physiotherapy, Yoga, Tai Chi, Heat/Ice | Improves mobility, strengthens supporting muscles, reduces stiffness |
| Pharmacological | NSAIDs, Gabapentinoids, SNRIs, Topical Lidocaine | Reduces inflammation or calms nerve signaling without heavy sedation |
| Psychological | Cognitive Behavioral Therapy (CBT), Mindfulness, ACT | Changes pain perception, reduces fear-avoidance, improves coping |
| Interventional | Nerve Blocks, Epidurals, Radiofrequency Ablation | Targets specific pain generators for temporary relief to enable therapy |
Note that opioids are rarely the first line of defense in this model. They may be used sparingly for breakthrough pain, but they are not the foundation. The foundation is active participation in your own recovery.
Setting Realistic Functional Goals
How do you apply the golden rule today? Start by defining what "better" looks like for you. Not "no pain," but "more life." Write down three specific goals. For example:
- "I want to walk my dog for 15 minutes without stopping."
- "I want to attend my daughter's school play without needing a rescue medication."
- "I want to sleep for six consecutive hours."
Then, work backward. What barriers stand in your way? Is it stiffness? Fear? Lack of knowledge? Share these goals with your healthcare provider. A good pain specialist will ask, "What do you want to do?" before asking, "Where does it hurt?"
Progress is rarely linear. You will have flare-ups. The golden rule teaches you to ride the wave of a flare-up rather than drown in it. Use heat, gentle movement, and relaxation techniques. Trust that the intensity will pass. Every time you successfully navigate a flare-up without giving up on your goals, you rewire your brain to see pain as manageable, not catastrophic.

The Role of Sleep and Stress
You cannot manage pain effectively if you are exhausted. Sleep deprivation lowers your pain threshold. When you don't sleep well, your brain’s amygdala (the fear center) becomes overactive, amplifying pain signals. Conversely, pain disrupts sleep. It is a feedback loop that must be broken.
Prioritizing sleep hygiene is not a luxury; it is a medical intervention. Keep a consistent schedule, limit screens before bed, and keep your room cool. Similarly, chronic stress releases cortisol and adrenaline, which can increase inflammation and muscle tension. Techniques like deep breathing, meditation, or even simple hobbies can lower this physiological arousal, indirectly reducing pain intensity.
When to Seek Help
If you are struggling to find balance, you are not alone. Chronic pain affects millions, and the old ways of treating it are being phased out. Look for providers who specialize in pain medicine, physiatry, or rheumatology, and who explicitly mention multidisciplinary care. Ask them directly: "Do you focus on improving function and quality of life?" Their answer will tell you everything you need to know about whether they follow the golden rule.
Is the golden rule of pain management applicable to acute pain?
The golden rule is primarily designed for chronic pain (lasting more than 3-6 months). For acute pain, such as post-surgery or trauma, the goal is still significant pain reduction to facilitate healing and immediate function. However, even in acute settings, doctors are increasingly cautious with opioids to prevent the transition to chronic pain.
Does following the golden rule mean I should never take pain medication?
No. Medication is a valuable tool in multimodal analgesia. The key is using the right medication for the right type of pain at the lowest effective dose. Non-opioid options like NSAIDs, acetaminophen, or nerve pain medications (gabapentin) are often preferred. Opioids may be used occasionally for severe flare-ups but are not recommended as a daily long-term solution due to risks of tolerance and dependence.
How do I explain this approach to family members who think I'm "just pushing through" pain?
Explain that pain is not just a sensation but a complex brain response. Tell them that avoiding movement makes the pain worse in the long run by weakening muscles. Frame your activities as "rehabilitation" rather than "ignoring pain." Ask them to support your functional goals, like cheering you on during a walk, rather than focusing on your grimaces or complaints.
What is the difference between CBT and traditional talk therapy for pain?
Traditional talk therapy often focuses on processing past emotions. Cognitive Behavioral Therapy (CBT) for pain is skills-based. It teaches you practical techniques to identify negative thought patterns (e.g., "This pain will last forever") and replace them with realistic ones ("This is uncomfortable, but I can cope"). It also includes behavioral experiments, like gradually increasing activity to prove to your brain that movement is safe.
Can exercise make chronic pain worse?
It can, if done incorrectly. "Pushing through" sharp pain can cause reinjury. However, gentle, graded exercise is essential. The key is pacing. Start with very low-intensity movements (like walking or swimming) and increase duration slowly. Some increased discomfort is normal, but it should settle within an hour or two. If pain spikes and lasts for days, you went too far and need to step back slightly.